Bursitis Of The Foot Pain
Overview
Calcaneal bursitis is seen somewhat frequently, particularly if the clinician has a predominantly musculoskeletal practice. No mortality is associated with calcaneal bursitis. Morbidity is associated with progressive pain and limping (antalgic gait) in patients who have not received adequate treatment. If chronic inflammation also affects the distal Achilles tendon, rupture of the tendon may occur. No race predilection has been documented. Calcaneal bursitis is observed in men and women. However, some increased risk may be incurred by women who wear high-heeled shoes. Calcaneal bursitis is commonly observed in middle-aged and elderly persons, the condition is also seen in athletes of all ages.Bursitis is a painful swelling of a small sac of fluid called a bursa. Bursae (plural of bursa) cushion and lubricate areas where tendons, ligaments, skin, muscles, or bones rub against each other. People who repeat the same movement over and over or who put continued pressure on a joint in their jobs, sports, or daily activities have a greater chance of getting bursitis.
Causes
Wearing poorly fitting or constrictive footwear can cause the heel to become irritated and inflamed. Shoes that dig into the back of the heel are the primary cause of retroachilles bursitis. Foot or ankle deformity. A foot or ankle deformity can make it more likely to develop retrocalcaneal bursitis. For example, some people can have an abnormal, prominent shape of the top of their heel, known as a Haglund's deformity. This condition increases the chances of irritating the bursa. A trauma to the affected heel, such as inadvertently striking the back of the heel against a hard object, can cause the bursa to fill with fluid, which in turn can irritate and inflame the bursa's synovial membrane. Even though the body usually reabsorbs the fluid, the membrane may stay inflamed, causing bursitis symptoms.
Symptoms
Pain at the back of the heel, especially when running uphill. Pain may get worse when rising on the toes (standing on tiptoes). Tenderness at the back of heel. Swelling at the back of heel.
Diagnosis
Bursitis is usually diagnosed after a careful physical examination and a full review of your medical history. If you garden and spend a lot of time on your knees, or if you have rheumatoid arthritis, tell your doctor, this information can be very helpful. During the physical exam, he or she will press on different spots around the joint that hurts. The goal is to locate the specific bursa that is causing the problem. The doctor will also test your range of motion in the affected joint. Other tests usually aren?t required to diagnose bursitis, but your doctor may suggest an MRI, X-ray or ultrasound to rule out other potential causes of pain.
Non Surgical Treatment
Gradual and progressive stretching of the Achilles tendon. Exercises to strengthen and support the ankle. Rest or reduced weight bearing activities. Immobilisation in a cast for 4-6 weeks for severe cases. Ice. Proper fitting and supportive footwear. Massage. Joint mobilisation. Anti-inflammatory medications: only if this does not have adverse results with the patient's current medication. Heel pads and heel lifts. Footwear Advice. Strapping and padding Orthoses/innersoles. The orthotics prescribed and designed by the podiatrists at the Heel and Arch Pain Clinic (affiliated with Beyond Podiatry) are made to align the foot in the correct posture. Surgery is indicated in severe cases when conservative treatment has not resolved the problem.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
Calcaneal bursitis is seen somewhat frequently, particularly if the clinician has a predominantly musculoskeletal practice. No mortality is associated with calcaneal bursitis. Morbidity is associated with progressive pain and limping (antalgic gait) in patients who have not received adequate treatment. If chronic inflammation also affects the distal Achilles tendon, rupture of the tendon may occur. No race predilection has been documented. Calcaneal bursitis is observed in men and women. However, some increased risk may be incurred by women who wear high-heeled shoes. Calcaneal bursitis is commonly observed in middle-aged and elderly persons, the condition is also seen in athletes of all ages.Bursitis is a painful swelling of a small sac of fluid called a bursa. Bursae (plural of bursa) cushion and lubricate areas where tendons, ligaments, skin, muscles, or bones rub against each other. People who repeat the same movement over and over or who put continued pressure on a joint in their jobs, sports, or daily activities have a greater chance of getting bursitis.
Causes
Wearing poorly fitting or constrictive footwear can cause the heel to become irritated and inflamed. Shoes that dig into the back of the heel are the primary cause of retroachilles bursitis. Foot or ankle deformity. A foot or ankle deformity can make it more likely to develop retrocalcaneal bursitis. For example, some people can have an abnormal, prominent shape of the top of their heel, known as a Haglund's deformity. This condition increases the chances of irritating the bursa. A trauma to the affected heel, such as inadvertently striking the back of the heel against a hard object, can cause the bursa to fill with fluid, which in turn can irritate and inflame the bursa's synovial membrane. Even though the body usually reabsorbs the fluid, the membrane may stay inflamed, causing bursitis symptoms.
Symptoms
Pain at the back of the heel, especially when running uphill. Pain may get worse when rising on the toes (standing on tiptoes). Tenderness at the back of heel. Swelling at the back of heel.
Diagnosis
Bursitis is usually diagnosed after a careful physical examination and a full review of your medical history. If you garden and spend a lot of time on your knees, or if you have rheumatoid arthritis, tell your doctor, this information can be very helpful. During the physical exam, he or she will press on different spots around the joint that hurts. The goal is to locate the specific bursa that is causing the problem. The doctor will also test your range of motion in the affected joint. Other tests usually aren?t required to diagnose bursitis, but your doctor may suggest an MRI, X-ray or ultrasound to rule out other potential causes of pain.
Non Surgical Treatment
Gradual and progressive stretching of the Achilles tendon. Exercises to strengthen and support the ankle. Rest or reduced weight bearing activities. Immobilisation in a cast for 4-6 weeks for severe cases. Ice. Proper fitting and supportive footwear. Massage. Joint mobilisation. Anti-inflammatory medications: only if this does not have adverse results with the patient's current medication. Heel pads and heel lifts. Footwear Advice. Strapping and padding Orthoses/innersoles. The orthotics prescribed and designed by the podiatrists at the Heel and Arch Pain Clinic (affiliated with Beyond Podiatry) are made to align the foot in the correct posture. Surgery is indicated in severe cases when conservative treatment has not resolved the problem.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
Contracted Toe Pain
 Overview
Overview
There are two different types of hammertoe. Flexible Hammer Toes. These hammer toes are less serious because they can be diagnosed and treated while still in the developmental stage. They are called flexible hammer toes because they are still moveable at the joint. Rigid Hammer Toes. This variety is more developed and more serious than the flexible condition. Rigid hammer toes can be seen in patients with severe arthritis, for example, or in patients who wait too long to seek professional treatment. The tendons in a rigid hammer toe have become tight, and the joint misaligned and immobile, making surgery the usual course of treatment.
Causes
Hammer toe results from shoes that don?t fit properly or a muscle imbalance, usually in combination with one or more other factors. Muscles work in pairs to straighten and bend the toes. If the toe is bent and held in one position long enough, the muscles tighten and cannot stretch out. Some other causes are diabetes, arthritis, neuromuscular disease, polio or trauma.
 Symptoms
Symptoms
The symptoms of hammertoe are progressive, meaning that they get worse over time. Hammertoe causes the middle joint on the second, third, fourth, or fifth toes to bend. The affected toe may be painful or irritated, especially when you wear shoes. Areas of thickened skin (corns) may develop between, on top of, or at the end of your toes. Thickened skin (calluses) may also appear on the bottom of your toe or the ball of your foot. It may be difficult to find a pair of shoes that is comfortable to wear.
Diagnosis
Your doctor is very likely to be able to diagnose your hammertoe simply by examining your foot. Even before that, he or she will probably ask about your family and personal medical history and evaluate your gait as you walk and the types of shoes you wear. You'll be asked about your symptoms, when they started and when they occur. You may also be asked to flex your toe so that your doctor can get an idea of your range of motion. He or she may order x-rays in order to better define your deformity.
Non Surgical Treatment
In many cases, conservative treatment consisting of physical therapy and new shoes with soft, spacious toe boxes is enough to resolve the condition, while in more severe or longstanding cases podiatric surgery may be necessary to correct the deformity. The patient's doctor may also prescribe some toe exercises that can be done at home to stretch and strengthen the muscles. For example, the individual can Hammer toe gently stretch the toes manually, or use the toes to pick things up off the floor. While watching television or reading, one can put a towel flat under the feet and use the toes to crumple it. The doctor can also prescribe a brace that pushes down on the toes to force them to stretch out their muscles.
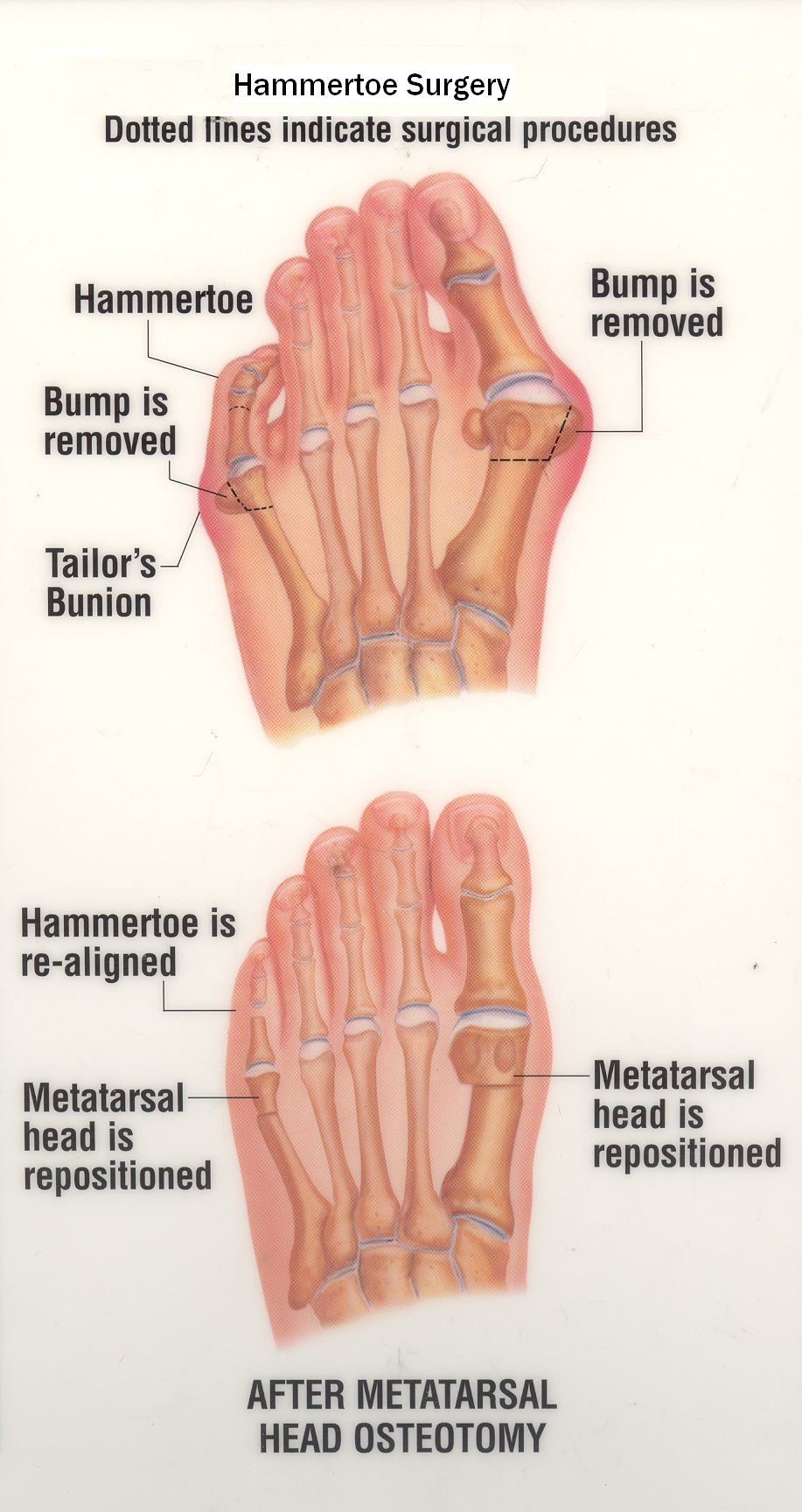
Surgical Treatment
Sometimes when the joints are removed the two bones become one as they are fused in a straightened position. Many times one toe will be longer than another and a piece of bone is removed to bring the toes in a more normal length in relation to each other. Sometimes tendons will be lengthened, or soft tissue around the joints will be cut or rebalanced to fix the deformity. Angular corrections may also be needed. The surgeon may place fixation in your foot as it heals which may include a pin, or wires.
 Prevention
Prevention
Preventing foot problems, including hammertoes, is often a matter of wearing the right shoes and taking care of your feet. Check your feet regularly for problems. This is especially true if you have diabetes or any other medical condition that causes poor circulation or numbness in your toes. If you do, check feet daily so that problems can be caught early on.
Hammertoe Correction Without Surgery
 Overview
Overview
A hammertoes is a toe that is bent because of a weakened muscle. The weakened muscle makes the tendons (tissues that connect muscles to bone) shorter, causing the toes to curl under the feet. Hammertoes can run in families. They can also be caused by shoes that are too short. Hammertoes can cause problems with walking and can lead to other foot problems, such as blisters, calluses, and sores. Splinting and corrective footwear can help in treating hammertoes. In severe cases, surgery to straighten the toe may be necessary.
Causes
The constant pressure a woman's foot receives in high-heeled shoes due to the force of gravity causes their feet to naturally slide down and press on the lowest point of the shoe so they are not able to receive enough space and stretch out. The result is an eventual distortion of the woman's toes. The deformity comes as a result of the shortening of muscles inside the toes because the toes become used to being in a bent position, prompting the muscles to fail to extend any further and become tightened and curbed. At first, toes may still be stretched out if poor footwear is not being worn, yet if the habit is persistent...the person's toes will eventually become used to the position they are constantly in and muscle fibers inside them will harden and refuse to stretch.
 Symptoms
Symptoms
The most obvious symptom of hammertoe is the bent, hammer-like or claw-like appearance of one or more of your toes. Typically, the proximal joint of a toe will be bending upward and the distal joint will be bending downward. In some cases, both joints may bend downward, causing the toes to curl under the foot. In the variation of mallet toe, only the distal joint bends downward. Other symptoms may include Pain and stiffness during movement of the toe, Painful corns on the tops of the toe or toes from rubbing against the top of the shoe's toe box, Painful calluses on hammertoes the bottoms of the toe or toes, Pain on the bottom of the ball of the foot, Redness and swelling at the joints. If you have any of these symptoms, especially the hammer shape, pain or stiffness in a toe or toes, you should consider consulting your physician. Even if you're not significantly bothered by some of these symptoms, the severity of a hammertoe can become worse over time and should be treated as soon as possible. Up to a point hammertoes can be treated without surgery and should be taken care of before they pass that point. After that, surgery may be the only solution.
Diagnosis
The treatment options vary with the type and severity of each hammer toe, although identifying the deformity early in its development is important to avoid surgery. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition.
Non Surgical Treatment
A person with hammer toes will be asked to practice some exercises for their toes to regain average structure and movement. The exercises usually involve stretching and strengthening their toes. The person may attempt to pick things up off the floor using only their toes. They may also stretch their toes on a regular basis by hand to ease them into straightening out. Another example of a physical exercise specifically for a person's toes involves crumpling a towel with the toes. The towel can lie underneath the person's feet and the person can use their toes to scrunch up the towel as they perform simple tasks such as reading a book or watching television.
Surgical Treatment
Surgery may be the treatment of choice if conservative approaches prove unsuccessful. Usually performed as an outpatient procedure, the specific surgery will depend on the type and extent of injury to the toe. Recovery my take several days or weeks and you may experience some redness, stiffness and swelling of the affected toe. Your physician will recommend taking it easy and to keep your foot elevated while you recover.
 Prevention
Prevention
Hammertoe can usually be prevented by wearing shoes that fit properly and give the toes plenty of room. Don?t wear shoes with pointed or narrow toes. Don?t wear shoes that are too tight or short. Don?t wear high-heeled shoes, which can force the toes forward. Choose shoes with wide or boxy toes. Choose shoes that are a half-inch longer than your longest toe. If shoes hurt, don?t wear them.
Bunions Symptoms
Overview
 Bunions, Corns, and Calluses are common foot ailments associated with improperly-fitted footwear. Please contact your family doctor or Podiatrist to ask them how Birkenstock footwear or arch supports can help treat your symptoms. Also, feel free to contact your local Birkenstock retailer about their healthy footwear recommendations. Birkenstock has many products that can help with Bunions, Corns, and Calluses. Bunions are a prominent bump on the inside of the foot around the big toe joint. Corns are an accumulation of dead skin cells usually found on the toes, forming thick hardened areas. They contain a cone-shaped core whose point can press on a nerve below causing pain. Calluses are also an accumulation of dead skin cells that harden and thicken over an area of the foot. They are the body?s defense mechanism against excessive pressure and friction. Calluses are normally found on the bottom of the foot, the heel, and/or the inside of the big toe.
Bunions, Corns, and Calluses are common foot ailments associated with improperly-fitted footwear. Please contact your family doctor or Podiatrist to ask them how Birkenstock footwear or arch supports can help treat your symptoms. Also, feel free to contact your local Birkenstock retailer about their healthy footwear recommendations. Birkenstock has many products that can help with Bunions, Corns, and Calluses. Bunions are a prominent bump on the inside of the foot around the big toe joint. Corns are an accumulation of dead skin cells usually found on the toes, forming thick hardened areas. They contain a cone-shaped core whose point can press on a nerve below causing pain. Calluses are also an accumulation of dead skin cells that harden and thicken over an area of the foot. They are the body?s defense mechanism against excessive pressure and friction. Calluses are normally found on the bottom of the foot, the heel, and/or the inside of the big toe.
Causes
Bunions may be hereditary, as they often run in families. This suggests that people may inherit a faulty foot shape. In addition, footwear that does not fit properly may cause bunions. Bunions are made worse by tight, poorly-fitting, or too-small shoes. Bunions may also happen due to inflammatory conditions such as arthritis. Anyone can get bunions, but they are more common in women. People with flat feet are also more likely to get bunions due to the changes in the foot caused by bunions. There is also a condition called adolescent bunion, which tends to occur in 10-to-15-year old girls.
Symptoms
Many people do not experience symptoms in the early stages of bunion formation. Symptoms are often most noticeable when the bunion gets worse and with certain types of footwear. These include shoes that crowd the toes and/or high-heeled shoes. When symptoms do occur, they may include physical discomfort or pain. A burning feeling. Redness and swelling. Possible numbness. Difficulty walking.
Diagnosis
A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen.
Non Surgical Treatment
There are many treatment options for bunions and they will vary with the type and severity of each bunion and will also depend on what is causing the symptoms. Bunions are almost always progressive and tend to get larger and more painful with time, how fast this happens may be a function of the fit of the footwear. The initial goal of treatment options is to relieve pressure on the bunion and any symptoms that may be present and to halt or slow the progression of the joint deformity. There is no effective may be "get rid off" a bunion without surgery. There are a number of things that individuals and Podiatrists can do to help the symptoms and slow (if not halt) progression. 
Surgical Treatment
Bunion surgery generally involves repositioning the maligned bones with a bone cut (osteotomy) and/or bone mending procedure (fusion). As such, the time it takes for bones to set or mend in the corrected position generally takes six weeks. Smokers and those in poor medical health may take longer to mend the bone. The biology of bone healing is about six weeks, that time frame can't be made quicker. What can be changed is the disability that one experiences while the bone is mending.
Overpronation Of The Feet
Overview
Too much of a good thing can be bad, and when it comes to pronation of the foot this is often the case. When the foot rolls too much during contact with the ground, the body weight is not cushioned effectively. The degree to which pronation occurs may be difficult to spot without someone observing how you run. It is easier to tell if a runner is pronating excessively when they are observed from behind rather than from above. When overpronation is only mild to moderate it may not be easy to spot without having a professional gait analysis performed..gif)
Causes
You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation.
Symptoms
Common conditions that develop with prolonged overpronation typically include plantar fasciitis, achilles tendonitis, shin splints, posterior tibial stress syndrome and even IT band syndrome. With long term neglect you may see the development of bunyons, foot deformities and early onset of hip and knee arthritis.
Diagnosis
Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.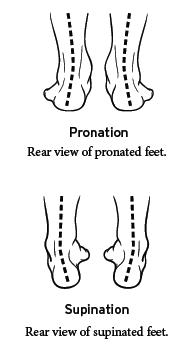
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Too much of a good thing can be bad, and when it comes to pronation of the foot this is often the case. When the foot rolls too much during contact with the ground, the body weight is not cushioned effectively. The degree to which pronation occurs may be difficult to spot without someone observing how you run. It is easier to tell if a runner is pronating excessively when they are observed from behind rather than from above. When overpronation is only mild to moderate it may not be easy to spot without having a professional gait analysis performed.
Causes
You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation.
Symptoms
Common conditions that develop with prolonged overpronation typically include plantar fasciitis, achilles tendonitis, shin splints, posterior tibial stress syndrome and even IT band syndrome. With long term neglect you may see the development of bunyons, foot deformities and early onset of hip and knee arthritis.
Diagnosis
Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Could I Care For Calcaneal Apophysitis At Home ?
Overview
Sever's disease is a common cause of heel pain in growing kids, especially those who are physically active. It usually occurs during the growth spurt of adolescence, the approximately 2-year period in early puberty when kids grow most rapidly. This growth spurt can begin any time between the ages of 8 and 13 for girls and 10 and 15 for boys. Sever's disease rarely occurs in older teens because the back of the heel usually finishes growing by the age of 15, when the growth plate hardens and the growing bones fuse together into mature bone. Sever's disease is similar to Osgood-Schlatter disease, a condition that affects the bones in the knees.
Causes
Children are at a higher risk of developing Sever's disease when they are in the early stages of a growth spurt. During times of growth, muscles and tendons become extremely tight. Movements during athletic activities like soccer, tennis, and gymnastics can put added force on the growth plate in the heel, which is pulled tight by the Achilles tendon. Over time, the growth plate becomes inflamed and painful. There are several other factors that can increase a child's risk of developing Sever's disease, including the following. Excessive pronation. Flat or high arches. Short Achilles tendon. Weight gain (which results in more force on the feet).
Symptoms
The symptoms of Sever?s disease occur in the heel and the foot, and may worsen with activity. Pain and stiffness can occur in one or both heels. Symptoms can include. Swelling in the heel. Redness in the heel. Antalgic gait (such as limping). Foot pain or stiffness first thing in the morning or while walking. Pain that is worsened by squeezing the heel.
Diagnosis
Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture.
Non Surgical Treatment
The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever's disease is a common cause of heel pain in growing kids, especially those who are physically active. It usually occurs during the growth spurt of adolescence, the approximately 2-year period in early puberty when kids grow most rapidly. This growth spurt can begin any time between the ages of 8 and 13 for girls and 10 and 15 for boys. Sever's disease rarely occurs in older teens because the back of the heel usually finishes growing by the age of 15, when the growth plate hardens and the growing bones fuse together into mature bone. Sever's disease is similar to Osgood-Schlatter disease, a condition that affects the bones in the knees.
Causes
Children are at a higher risk of developing Sever's disease when they are in the early stages of a growth spurt. During times of growth, muscles and tendons become extremely tight. Movements during athletic activities like soccer, tennis, and gymnastics can put added force on the growth plate in the heel, which is pulled tight by the Achilles tendon. Over time, the growth plate becomes inflamed and painful. There are several other factors that can increase a child's risk of developing Sever's disease, including the following. Excessive pronation. Flat or high arches. Short Achilles tendon. Weight gain (which results in more force on the feet).
Symptoms
The symptoms of Sever?s disease occur in the heel and the foot, and may worsen with activity. Pain and stiffness can occur in one or both heels. Symptoms can include. Swelling in the heel. Redness in the heel. Antalgic gait (such as limping). Foot pain or stiffness first thing in the morning or while walking. Pain that is worsened by squeezing the heel.
Diagnosis
Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture.
Non Surgical Treatment
The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Posterior Tibial Tendon Dysfunction Cause And Treatment
Overview
Adult acquired flatfoot deformity (AAFD or AAF) is a progressive, symptomatic deformity resulting from gradual stretch of the posterior tibial tendon as well as other ligaments supporting the arch of the foot. AAFD develops after skeletal maturity, May also be referred to as posterior tibial tendon dysfunction (PTTD), although due to the complexity of the disorder AAFD is more appropriate. Significant ligamentous rupture occurs as the deformity progresses. Involved ligaments include the spring ligament, the superficial deltoid ligament, the plantar fascia, and the long and short plantar ligaments. Unilateral AAFD is more common than bilateral AAFD. 
Causes
As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Symptoms
Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain.
Diagnosis
First, both feet should be examined with the patient standing and the entire lower extremity visible. The foot should be inspected from above as well as from behind the patient, as valgus angulation of the hindfoot is best appreciated when the foot is viewed from behind. Johnson described the so-called more-toes sign: with more advanced deformity and abduction of the forefoot, more of the lateral toes become visible when the foot is viewed from behind. The single-limb heel-rise test is an excellent determinant of the function of the posterior tibial tendon. The patient is asked to attempt to rise onto the ball of one foot while the other foot is suspended off the floor. Under normal circumstances, the posterior tibial muscle, which inverts and stabilizes the hindfoot, is activated as the patient begins to rise onto the forefoot. The gastrocnemius-soleus muscle group then elevates the calcaneus, and the heel-rise is accomplished. With dysfunction of the posterior tibial tendon, however, inversion of the heel is weak, and either the heel remains in valgus or the patient is unable to rise onto the forefoot. If the patient can do a single-limb heel-rise, the limb may be stressed further by asking the patient to perform this maneuver repetitively.
Non surgical Treatment
A patient who has acute tenosynovitis has pain and swelling along the medial aspect of the ankle. The patient is able to perform a single-limb heel-rise test but has pain when doing so. Inversion of the foot against resistance is painful but still strong. The patient should be managed with rest, the administration of appropriate anti-inflammatory medication, and immobilization. The injection of corticosteroids is not recommended. Immobilization with either a rigid below-the-knee cast or a removable cast or boot may be used to prevent overuse and subsequent rupture of the tendon. A removable stirrup-brace is not initially sufficient as it does not limit motion in the sagittal plane, a component of the pathological process. The patient should be permitted to walk while wearing the cast or boot during the six to eight-week period of immobilization. At the end of that time, a decision must be made regarding the need for additional treatment. If there has been marked improvement, the patient may begin wearing a stiff-soled shoe with a medial heel-and-sole wedge to invert the hindfoot. If there has been only mild or moderate improvement, a longer period in the cast or boot may be tried. .jpg)
Surgical Treatment
Good to excellent results for more than 80% of patients have been reported at five years' follow up for the surgical interventions recommended below. However, the postoperative recovery is a lengthy process, and most surgical procedures require patients to wear a plaster cast for two to three months. Although many patients report that their function is well improved by six months, in our experience a year is required to recover truly and gain full functional improvement after the surgery. Clearly, some patients are not candidates for such major reconstructive surgery.